

Crohn’s disease and ulcerative colitis are the two most common autoimmune inflammatory bowel diseases (IBD). IBDs have no cure, but there are treatments to control the disease. Guarantee the patient’s quality of life: the diagnosis and management of the disease will be essential.
What is inflammatory bowel disease?
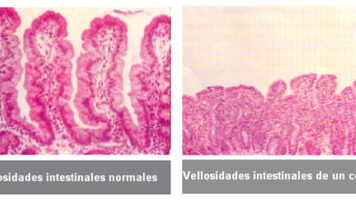
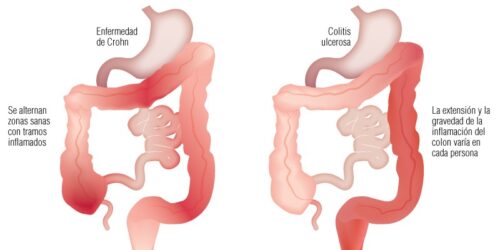
IBD is a chronic disease in which the immune system attacks the body itself and causes inflammation and injury to the intestine. Crohn’s disease can affect any part of the digestive tract from the mouth to the anus and colitis to the large intestine. These diseases cause different affectations to the intestinal tissue: inflammation or accumulation of scar tissue that can cause obstruction, development of lesions (ulcers and fistulas), and malabsorption of nutrients.
The cause of these diseases is unknown. There is a combination of genetic and environmental factors that cause an abnormal response to the immune system of the gastrointestinal tract. It is common in developed countries and affects any age, but is most common between 15 and 30 years of age.
What are the symptoms?
The disease works in the form of intermittent outbreaks, that is, periods of severe symptoms followed by periods of remission (mildly symptomless or asymptomatic) that can last for weeks or years (not knowing when it will occur).
The initial symptoms are abdominal pain accompanied by diarrhea, although they will vary according to what part of the intestine is affected and its severity.
- Crohn’s disease usually produces: bulky diarrhea, loss of appetite and weight, fever, fistulas, canker sores, vomiting, feeling full and delayed childhood growth.
- In ulcerative colitis it is more common to have diarrheal stools of less volume, but more frequent, with blood, pus and mucus, feeling of incomplete evacuation and urgency of the stools.
In both cases, because the intestine is affected and nutrients are not properly absorbed, patients can present with osteoporosis, fatigue and lack of concentration, anemia and malnutrition. Other secondary alterations occur at the dermal level (rashes or skin lesions), articular (arthritis), liver (only in the case of colitis) and in the eyes (uveitis).
How is it diagnosed?
Various tests are used to diagnose IBD, first going through a medical history review and physical examination; and later by some other complementary test (digestive or analytical endoscopy of blood and excrement or imaging tests).
What does the treatment consist of?
Treatment will aim to control inflammation, correct dietary deficiencies, and alleviate symptoms, since the disease has no cure. Sometimes the disease can go into remission on its own, making it difficult to know if a treatment has been effective.
The application of the treatment will depend on the severity of the disease and its location in the intestine. At the pharmacological level, some of the prescribed medications are anti-inflammatories, antibiotics, antidiarrheals and medications that suppress the immune system. Abandoning treatment can cause a relapse or a poor evolution of the disease. Sometimes (more often in Crohn’s) surgery is needed that can correct perforations, bleeding, or intestinal obstructions.
On the other hand, maintaining a healthy lifestyle is essential to manage the disease well. Being physically active, not smoking or consuming toxic substances and following a healthy diet. Dietary treatment is the key to a correct evolution of the disease and it is important to be guided by a qualified professional.
How should the diet be?
Diet is not the cause of inflammatory bowel disease, but there are foods that can make symptoms worse.
The goal of the diet is to decrease the antigenic load, reduce the inflammatory mediators and provide all the nutrients necessary for tissue repair and avoid nutritional deficits. If it is not done correctly, there is a 20% to 85% risk of malnutrition due to loss of appetite and intestinal malabsorption. A nutritionist must supervise it.
The diet must be healthy, balanced and adapted to the needs of the individual and to the treatments applied (drugs and / or surgery). Some of the recommendations are:
- Eat in small quantities
- Avoid extreme food temperatures
- Reduce and adapt the intake of fats and simple sugars
- Adapt the type of fiber
- Eliminate lactose in case of intolerance
- Ensure correct hydration with specific isotonic drinks
- Avoid precooked, irritating, sweetening and flatulent foods
- Avoid foods rich in histamine if the DAO enzyme has been affected (very common in both diseases)
What is the relationship between IBD and the deficit of DAO activity?
It has been observed that in IBD patients the activity of the DAO enzyme is 50% lower compared to healthy patients, this data supports the hypothesis that individuals with a mutation in the DAO enzyme can show susceptibility to ulcerative colitis; as well as an increased secretion of histamine in the intestine. DAO would be a useful marker for predicting the risk of recurrence or complications in IBD.
Damage to the intestinal mucosa caused by, for example, gastroenteritis, irritable bowel syndrome, or gastrointestinal surgery or drug treatment may reduce DAO activity.
Two of the big problems IBD patients face are resistance to treatments and side effects. Among these complications, a deficiency of DAO enzyme activity may occur due to the application of some aggressive pharmacological treatment that may cause intestinal malabsorption. In these cases, dietary treatment should be performed to improve the quality of life of the patient.
What is the prognosis?
Like many other disorders, IBD has a great psychosocial impact, so understanding and education are the most important tools to manage the disease, improve symptoms and prevent complications.
BIBLIOGRAPHY
- https://my.clevelandclinic.org/health/diseases/9357-crohns-disease
- https://www.alimente.elconfidencial.com/bienestar/2019-05-19/colitis-ulcerosa-enfermedad-de-crohn_2005010/
- https://www.accucatalunya.cat/ca/malalties/malalties-inflamatories-intestinals-mii/
- https://www.clinicbarcelona.org/ca/asistencia/malalties/malaltia-inflamatoria-intestinal/viure-amb-la-malaltia
- Schnedl WJ, Lackner S, Enko D, Schenk M, Mangge H, Holasek SJ. Non-celiac gluten sensitivity: people without celiac disease avoiding gluten—is it due to histamine intolerance? Inflamm Res. Springer International Publishing; 2018;67(4):279-84.
- Honzawa Y, Nakase H, Matsuura M, Chiba T. Clinical significance of serum diamine oxidase activity in inflammatory bowel disease: Importance of evaluation of small intestinal permeability. Inflamm Bowel Dis. 2011;17(2):23-5.
- Fabisiak A, Wlodarczyk J, Fabisiak N, Storr M, Fichna J. Targeting histamine receptors in irritable bowel syndrome: A critical appraisal. J Neurogastroenterol Motil. 2017;23(3):341-8.



Hi my name is Duane. I have suspected chrons. 3 years before diagnosis. I suffer histamine intolerance so severe I can’t sleep.
Is there any help.
Hi Duane,
Of course, contact a specialist who can provide you with a dietary treatment.
Greetings!